It sounds so simple: losing 10 kilos in a year by giving yourself an injection once a week or every day. This is supposedly achievable with drugs like Ozempic ®, Wegovy ® or Mounjaro ®. They have been generating a lot of buzz, especially on social media, where they are often hailed as miracle cures for weight loss. But is that actually true?
In this episode of "Ziel mir keng!", we take a closer look at so-called "weight-loss jabs". How well do these treatments work? Who are they suitable for? And could they help tackle rising global obesity?
For this video, we were advised by researcher Dr Hanen Samouda, PhD, from the Luxembourg Institute of Health (LIH). She researches obesity at the LIH and is also the President of LASO, the Luxembourg Association for the Study of Obesity.
When it comes to obesity, it is not just about carrying extra weight or fitting a beauty ideal. In fact, the World Health Organization (WHO) recognises obesity as a disease and describes it as a global public health crisis.
More specifically, obesity is a complex, chronic, and multifactorial condition. It is linked to many other health problems, such as type 2 diabetes, cardiovascular disease, cancer, and muscular or psychological disorders.
According to researcher Dr Hanen Samouda from the LIH, effective obesity treatment starts with treating the disease itself. From there, the goals are to prevent related illnesses and improve public health overall.
But unfortunately, obesity is on the rise worldwide. In 1990, 8% of adults globally were living with obesity. By 2022, that number had doubled to 16%.
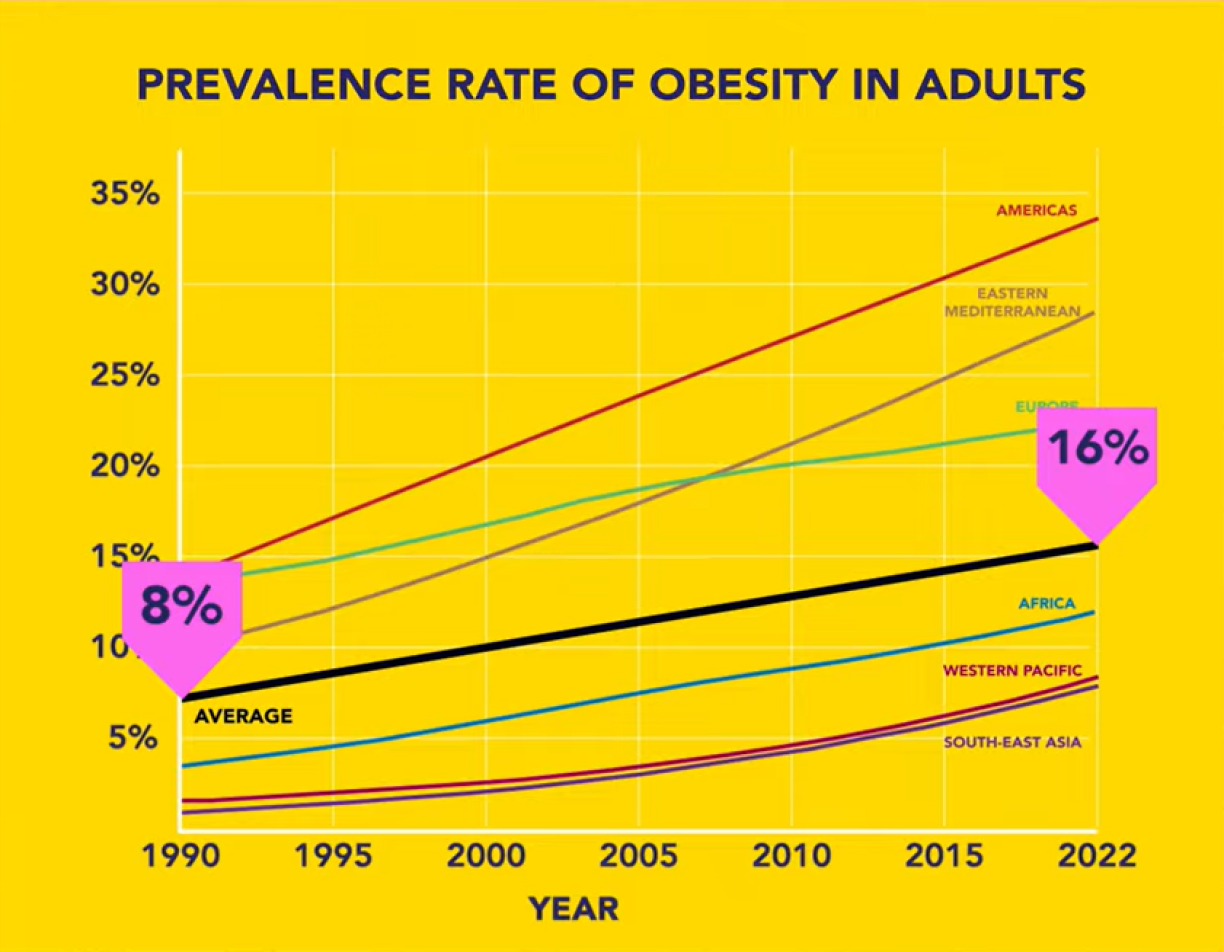
Luxembourg currently has similar rates. When you include children and adolescents, more than one billion people worldwide now have obesity. If we also account for pre-obesity or being overweight, over 2.5 billion people are affected globally.
Incidentally, cases of obesity among children and adolescents quadrupled between 1990 and 2022! Obesity at a young age isn’t just an immediate health risk – it has lasting consequences. Children with obesity are very likely to become adults with obesity, and they face a higher risk of developing illnesses earlier in life. On top of this, they experience additional negative psychosocial consequences: obesity affects school performance and quality of life, exacerbated by stigmatisation, discrimination and bullying.
The number of people affected is often determined using the BMI, or Body Mass Index. BMI is calculated based on a person’s weight and height. Someone is considered pre-obese or overweight if they have a BMI from 25 to < 30 kg/m². Obesity is defined as having a BMI of 30 kg/m² or higher.
For example: a person who is 1.75 metres tall would be considered overweight according to their BMI starting at around 77 kilos. From 93 kilos, they would be classified as obese.
BMI has the advantage of being easy to calculate. However, it often falls short: body fat percentage is more important than weight, along with other indicators, or indeed a patient’s overall health. Some athletes with lots of muscle, for instance, might have a high BMI too, but that doesn’t mean they have health problems because of it. That’s why other measurements are important too, such as waist size, physical and mental health markers, and how well someone functions in everyday life.
How exactly obesity should be defined and diagnosed is still being debated, even among experts. But one thing is clear: the focus is shifting away from weight alone and toward the patient's overall health.
Unfortunately, people with obesity are often stigmatised. Harmful prejudices persist, such as the idea that they simply lack willpower.
But some people are biologically more prone to putting on weight, due to differences in hunger, satiation, and energy regulation – all of which are influenced by genetics, brain function, and hormones.
At the same time, not everyone has equal access to healthy food, a healthy environment, time for exercise, or good healthcare. So it is not true that everyone starts from the same place. What’s more, once a person has obesity, it actually changes how their body works, e.g. their feelings of fullness, hunger, etc. So if someone with obesity develops disordered eating patterns, that’s often a consequence of the disease itself, which in turn makes the problem worse.
There are a lot of people who genuinely struggle to manage their weight and get healthy.
And then Ozempic® entered the scene.
This drug was actually developed for people with diabetes, to help regulate their blood sugar. But during trials, researchers discovered that they also lost weight. And not just a little bit.
That’s why, after further studies, medicines containing the same active ingredient as Ozempic (Wegovy®), along with others containing similar active ingredients (e.g. Mounjaro®), were also approved for treating excess weight and obesity.
In Luxembourg, Ozempic® is only authorised for the treatment of diabetes, while Wegovy® and Saxenda® are approved specifically for obesity or pre-obesity.
Depending on the study, patients with obesity lost between 10 and 20% of their body weight over one year*. This was always in combination with nutritional therapy and exercise.
*All references are listed at the end of the article.
To put that in perspective: people who are overweight and manage to stick with lifestyle changes over a similar period typically lose about 5-10%. After stomach-reduction surgery, the figure is 20% or more*. So 10-20% isn’t bad, is it?
But how do these jabs actually work?
The term "weight-loss jab" isn’t entirely accurate. They don’t destroy fat cells. Think of them more as "anti-hunger jabs". They contain active ingredients – like semaglutide – that mimic hormones (GLP-1), which make you feel full after a meal and regulate your blood sugar.
This class of medicines is therefore called GLP-1 agonists, and they work on the level of the body and the brain:
In simple terms: the medication makes you less hungry. You eat less. You lose weight.
But are these jabs actually a game-changer? After all, they could help a lot of people with obesity, and prevent numerous diseases worldwide, couldn’t they?
Indeed, studies involving people with obesity and excess weight have shown significant health improvements. The risk of a stroke or heart attack, for example, dropped by 20%, and the risk of developing diabetes fell by 66%.
These medications can also, among other things, lower blood pressure and reduce inflammation, support heart health, and decrease liver fat – all of which can improve quality of life for people with obesity. Recent research also points to benefits for joint pain, brain health, and other issues linked to being overweight.
Researchers have also conducted a modelling study. If every overweight or obese adult in the US were given these medications for life, the number of people with obesity would be cut in half after just two years. On top of that, each year would see 26 million fewer cases of diabetes, 13 million fewer cases of heart disease, and 5.5 million fewer premature deaths.
However, there are also side effects.
The most common ones include stomach aches, nausea, vomiting, diarrhoea, or constipation.
These tend to happen at the start of treatment or when the dose is increased. For many people, they improve with the help of medical nutritional therapy.
There are also rare, but more serious side effects, such as:
What's more, we don’t yet know whether other side effects might appear with long-term use.
Studies also show that once patients stop the injections, many regain at least some of the weight*. And much of the progress on blood pressure or blood sugar levels gradually slips back to where it started.
This reflects the fact that obesity is a chronic, recurring disease that requires long-term treatment.
These medications are no miracle cure that works in isolation. They can be part of an evidence-based, personalised therapy built on three pillars:
1)Pharmacotherapy
2) Surgery – e.g. stomach reduction
And 3) psychological support, medical nutrition therapy, and physical activity
The goal is always the same: improving quality of life and health.
But what about people who are "only" carrying a few extra kilos and are otherwise healthy? And who might want to turn to these medications simply to fit a certain beauty ideal?
In those cases, these medications should not be prescribed.
Here, the balance of risks versus benefits looks quite different. These individuals would be exposing themselves to potential side effects without necessarily gaining any real health benefits.
Because the medications were tested on obese patients, it is also unclear whether they might cause additional side effects in people of a normal weight.

Are medications like Wegovy® or Mounjaro® a game-changer or just nonsense?
Neither. They aren’t miracle cures, and they aren’t for everyone. But they are an important step forward and another tool for managing obesity, which is a chronic, complex disease carrying many other health risks.
These drugs can effectively support patients with obesity in improving their health. But they don't work in isolation.
They need to be considered as part of an evidence-based, long-term, and personalised therapy – one that also takes potential side effects into account. It’s crucial that this is done under proper medical supervision.
To what extent they can help fight the global public health crisis remains to be seen. It depends, among other things, on how obesity is managed in the future – and on whether these medications will be reimbursed, as is the case for other chronic illnesses. That discussion is currently ongoing.
At the moment, these drugs are still quite expensive. Not everyone in the world can afford them. Additionally, other aspects must be addressed alongside the drugs to prevent patients from regaining a significant amount of weight once treatment stops.
For people who are merely chasing a beauty ideal, lifestyle changes and a healthier relationship with body image remain the first option for improving their wellbeing and health.
Authors: Michèle Weber and Jean-Paul Bertemes (FNR)
Advice and peer-review : Dr Hanen Samouda, PhD (LIH)







